

Urinary catheter (UC) insertion is an important part of the management of several medical and surgical conditions. Some 15-25% of patients admitted to hospital have UCs inserted at some point (Saint and Chenoweth, 2003; Schumm and Lam, 2008; Bootsma et al, 2013; Loveday et al, 2014). Evidence suggests that 43.9-54% of these patients are given UCs inappropriately (Gokula et al, 2004; Holroyd-Leduc et al, 2005; Hazelett et al, 2006; Bootsma et al, 2013).
The longer a UC remains in the bladder the higher the risk of the patient developing bacterial infections (Majumder et al, 2014). A UC should therefore be inserted as a last resort after all alternatives have been exhausted, and removed as soon as possible (Pratt et al, 2007; Loveday et al, 2014; Royal College of Nursing (RCN), 2019).
This article discusses a thematic literature review of UC use from 2013 to 2018 and concentrates on three main risks:
- Infections
- Increased length of stay in hospital
- Death.
It was completed as part of a broader thematic review of UCs. The article provides a brief background to UCs, an account of the databases or methodology used for the literature review, and the findings. It then discusses and summarises recommendations in relation to current practice.
Background and overview
UCs are inserted for short-term or long-term purposes (Bardsley, 2015). They are used mainly as a short-term measure in the clinical area to relieve retention of urine (Meddings et al, 2014). A short-term UC is a catheter that is left in place for 14 days or fewer from the day of insertion, according to the European Association of Urology Nurses (EAUN, 2012). Others recommend that short-term UCs should remain in place for up to 7 days only (Yates, 2016). The EAUN suggests that the indication for inserting a UC will determine whether it is used as a short-term or long-term measure (EAUN, 2012; National Clinical Guideline Centre, 2012).
The longer a catheter remains in situ, the higher the risk of catheter-associated urinary tract infections (CAUTIs) developing (Jain et al, 1995; Gardam et al, 1998; Loveday et al, 2014; Majumder et al, 2014). The daily increase in risk of developing bacteria in the urine is 3-7% for a patient with a catheter, so total risk rises with the length of time that a device remains in place (Loveday et al, 2014, Al-Hazmi, 2015, Clayton, 2017).
UCs are also strongly linked to increased morbidity and mortality and a longer hospital stay, as well as higher hospital costs (Quinn, 2015; Richards et al, 2017). CAUTIs resulted in 45 717 extra bed-days in the NHS and 1467 deaths, with an estimated annual cost of £54.4 million for adult inpatients admitted in 2016-2017 (Smith et al, 2019). Each UC prevented could save about £30 in direct hospital costs per catheter and about £112 in quality-adjusted life-years (QALYs) (Smith et al, 2019). While the use of catheters cannot often be avoided, it is imperative that high standards of infection prevention and control are employed to reduce morbidity (Department of Health (DH), 2015).
Method
A literature search was used to identify studies on patients discharged from acute hospitals with short-term urinary catheters. Various databases were searched between May and October 2018, using Healthcare Databases Advanced Search (HDAS). The databases included the British Nursing Index (BNI), Medline and the Cumulative Index for Nursing and Allied Health Literature (CINAHL), as well as the Cochrane Library for Systematic Reviews. An email alert was set on HDAS from 25 May 2018 for an update on current research studies and reviews throughout the span of the search period. The library search at De Montfort University and Google Scholar were used to search the topic for conference reports and thesis. Some official websites, such as those of the EAUN, RCN, National Institute for Health and Care Excellence (NICE) and the Royal College of Physicians, were searched for guidelines and updated recommendations and reviews. The reference lists of selected journals, articles, guidelines and research studies were also searched manually.
The Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) flowchart was used to refine the results (Figure 1).
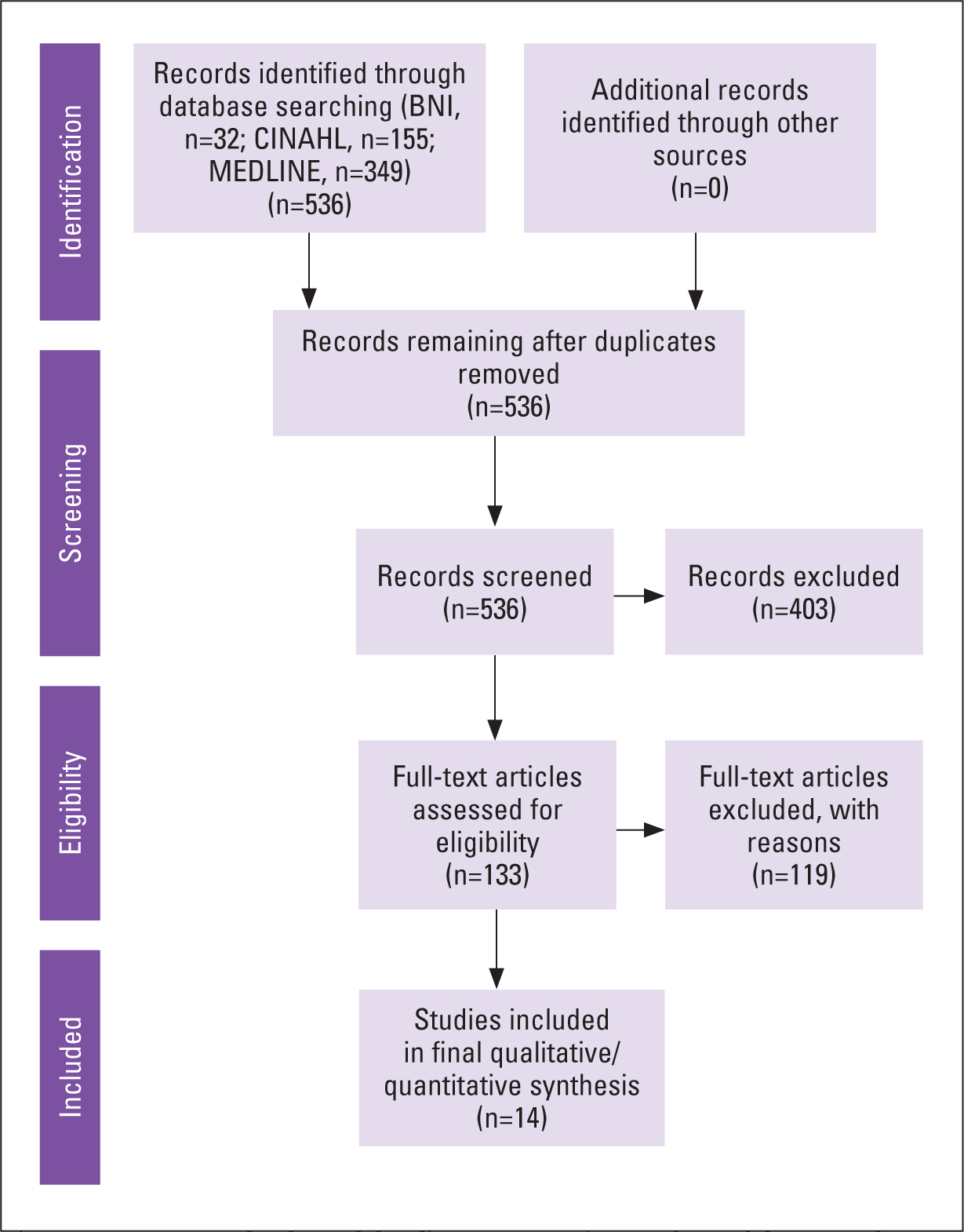 Fig 1. PRISMA method used for literature review
Fig 1. PRISMA method used for literature review
Findings
Catheter-associated urinary tract infections
A CAUTI occurs when bacteria travel through the lumen of the UC to the bladder (Carter et al, 2014). Ansell and Harari (2017) found that 34% of their study group developed catheter-related infections, and 21% developed life-threatening septicaemia in research that aimed to identify UC-related visits to the emergency department. Other studies, such as Eng (2017), found that 69 (58%) out of 118 urinary tract infections (UTIs) were related to UC, and 55 (10.5%) patients out of 524 with a UC in place developed a UTI in a study by Girard et al (2017). Although Girard et al (2017) found that the patients in their study had other implicating risk factors, such as a stay in a rehabilitation facility, female sex and immunosuppression, these 55 (10.5%) patients developed the UTI as direct a result of having a UC in situ.
Ansell and Harari (2017) suggested the need for more responsive community services for patients with UC, whereas Eng (2017) advocated implementing new measures to reduce the incidence of CAUTIs. These suggestions reaffirm the need for UCs to be monitored adequately and removed when no longer required. The Health and Social Care Act 2008 code of practice (DH, 2015) urges providers to establish a system that safeguards, monitors and protects patients from any form of risk, including infections. Although clinical areas have documentation for catheter care, and the expectation is that this is updated daily, in the authors' experience there is still a lack of critical challenge by healthcare workers in terms of the need for insertion, monitoring and removal of UCs.
Barbadoro et al (2015) aimed to establish the epidemiology of CAUTI through an active surveillance programme involving patients who were catheterised for at least 48 hours and monitored until discharge; 6.2% of the patients developed a CAUTI. The study highlighted the importance of hand hygiene and aseptic catheter insertion techniques in reducing CAUTI. In addition, a study by Daniels et al (2014) confirmed that 5.7% of patients with UC developed a CAUTI. In a retrospective study by Meddings et al (2014), 216 (74%) out of the 294 patients whose records were reviewed had a UC, and 5.8% met the criteria for CAUTI in the National Healthcare Safety Network American survey (Meddings et al, 2014).
Although the percentages of patients who developed CAUTI in the studies by Barbadoro et al (2015), Daniels et al (2014) and Meddings et al (2014) were not as high as in the studies by Eng (2017) and Ansell and Harari (2017), there is still enough evidence to suggest that UCs are associated with an increased risk of infection, and this can be life threatening. Evidence from the NHS safety thermometer suggests that more than 270 cases of Escherichia coli bacteraemia are associated with UCs, with CAUTI costing the NHS about £1 billion a year (Mantle, 2015). The current estimation, however, is £54.4 million a year (Smith et al, 2019). Darbyshire et al (2015) suggested that this reduction follows a change in culture that encourages health professionals to ensure UCs should be removed if not required, much in line with the Health and Social Care Act 2008 code of practice (DH, 2015).
Early removal of UCs has its own risks. A study by Nguyen et al (2016) found that early removal of a UC has the potential to cause catheter-related complications such as urinary retention. Nevertheless, the recommendation remains that UCs should be removed as early as possible to prevent CAUTI, while being mindful of other possible complications.
Some studies have implicated other factors, apart from the presence or absence of catheters, in the development of CAUTI. Powers (2016) investigated whether there was a relationship between CAUTI and breaking the closed drainage system of UCs, using an aseptic procedure. In an 8-month period there were 53 documented breaks in the urinary drainage system. There were 28 total cases of CAUTI overall during this same period. Only four patients with a system break developed a CAUTI (7.5%). In almost 93% of the patients where aseptic techniques were used for breaks in the drainage system, no CAUTIs occurred. A follow-up evaluation after a year also indicated no CAUTI where there had been aseptic breaks in drainage systems. It is therefore important to adhere to strict infection prevention measures to prevent CAUTI.
Length of stay and mortality
CAUTIs were found to be significantly associated with higher 7-day mortality rates in to a study by Melzer and Welch (2013). In this study, 559 bacteraemia episodes occurred in 437 patients, with 90 deaths (20.6%) at 7 days and 153 deaths (35.0%) at 30 days. The study recommended that efforts to reduce these infections should be a priority. Another study, by Daniels et al (2014), found a mortality rate of 3.9% compared to 2.0% in patients without CAUTI. In addition, 30-day mortality was associated with bacteraemia or fungaemia in patients with UC infections, which were often associated with E. coli (Melzer et al, 2015). Deaths associated with UC-related infections were significantly higher than those associated with intravascular devices. The recommendation was that a greater emphasis should be placed on preventing infections caused by UCs, which was reinforced by Powers (2016).
In addition to possible infections and death caused by UCs, there is also the potential of a longer hospital stay for patients with catheter-related complications who survive the infection. This was confirmed by Barbadoro et al (2015), who found that patients with CAUTI stayed in hospital for 4 days longer than average.
Weaknesses and strengths of the studies and reviews
Most of the studies were completed retrospectively using documentary evidence from medical records, which meant that the information for the study was readily available, easily accessible and cheap. This is also a permanent source of data which can be checked and validated, as suggested by Denscombe (2017).
The quantitative nature of the studies meant that documentary evidence and questionnaires were often used, thus eliminating researcher bias, which is often associated with methods such as face-to-face interviews (Kumar, 2014). The validity of information could be evaluated using the four-point check of authenticity, representativeness, meaning and credibility as advocated by Denscombe (2017).
On the other hand, the findings of most of these studies relied heavily on the quality of documentation in the clinical records, which in the case of urinary catheters is sometimes inadequate (Holroyd-Leduc et al, 2005; Welden, 2013). There was little information regarding comorbidities in the patients who were involved in the studies, which could have influenced outcomes.
Discussion
There is ample evidence to suggest that there is a direct relationship between UCs and the development of UTIs, increased length of stay and mortality. There is therefore the need for vigilance and adherence to protocols and education for health professionals and patients to ensure UCs are monitored and removed as soon as possible.
Although catheters ought to be removed as early as possible, healthcare workers should be mindful that, if they are removed too early, complications such as urinary retention could develop. It is important to note that, although UCs by themselves may be a source of infection, a break in the closed drainage system of the catheter without appropriate aseptic techniques can increase the risk of infection. Pre-existing comorbidities can also influence the risk of developing infection from a UC.
Two recent studies by Eng (2017) and Ansell and Harari (2017) in two different healthcare systems consistently showed a high incidence of CAUTI at 58% and 34% respectively. This seems to indicate that, irrespective of healthcare system, UCs pose risks to patients and hence there is a need for vigilance.
Various literature, including Bardsley (2009), has said that the most effective ways to reduce CAUTIs are having the need for UCs reviewed by health professionals, and for UCs to be removed when no longer required. Galiczewski (2016) demonstrated that interventions that included specific criteria for catheter use, daily review of catheter necessity and removal of the catheter before day 7 were effective in reducing catheter-related infections. Murphy et al (2014) suggested that more work is needed to establish when the initial placement of a urinary catheter is appropriate for patients to better understand when UCs are overused.
There is the need to continually create awareness, empower staff and engender a sense of ownership in relation to UC use among all health professionals. The development of policies for UC insertion, UC selection, UC avoidance, daily review and reduction of UC days, as well as educational programmes were highlighted by Chenoweth and Saint (2013) as measures required to reduce CAUTIs.
There have been several educational programmes and interventions to raise awareness, increase health professionals' knowledge and facilitate improvement in catheter care (Oman et al, 2012; Yoon et al, 2013; Quinn, 2015; Clayton, 2017; Parker et al, 2017; Richards et al, 2017; Davies et al, 2018). Some of the studies concerned an educational programme twice a year for health professionals along with the introduction of a daily checklist for UCs (Menegueti et al, 2019). This approach resulted in the mean rates of UC utilisation falling from 73.1% before the education programme to 45.6% afterwards. The incidence of CAUTIs before and after the programme were 14.9 per 1000 catheter-days and 1.1 per 1000 catheter-days respectively.
Similarly, the implementation of a CAUTI prevention bundle, which included indications, insertions, reviews and removal, as well as standardising the practice of collecting urine specimens, reduced the number of patients who received a UC from 25% to 16%. The rate of CAUTI also reduced by over one-third, from 4.07 to 2.56 per 1000 catheter-days (Davies et al, 2018). A multimodal approach, concentrating on teaching sessions for health professionals, surveillance systems and urinary catheterisation reminders, as well as feedback from the practitioners, also resulted in a decreased urinary catheterisation rate from 27.8% to 16.9%, and a reduction in CAUTI rate per 1000 patient-days from 5.5 to 2.8 (Ternavasio-de La Vega et al, 2016). Implementing a nurse-driven approach that used the HOUDINI guidelines (Table 1) to empower nurses to care for and remove UCs resulted in catheter-days falling from 679 to 625 and the catheter utilisation ratio improved from 0.19 to 0.17, although there was no incidence of CAUTI during the study period (Ballard, 2018).
Table 1. HOUDINI guidelines for urinary catheter removal and care
| Catheter removal | |
| This is a nursing process. You do not need a physician order to remove a urinary catheter that falls under HOUDINI guidelines. If any of the criteria below are met, do not remove the urinary catheter | |
| HOUDINI stands for: |
|
| Catheter care | |
| Urinary catheter care twice a day | Using soap and warm water, clean the perineum thoroughly from front to back |
| Always keep urinary bag below level of the bladder | eg during travel, head CTs, when working with physical therapy/occupational therapy and when transferring a patient from bed to chair |
| Obtain a urine culture |
|
| Document the process | Make sure all documentation is complete and accurate (ie twice-daily catheter care is charted and the date of placement of urinary are entered on assessment flowsheet) |
| Education | |
| Training/CPD | Complete online module for CAUTI reduction by a specific date |
Registered nurses and healthcare assistants could be empowered not only to document all patients with catheters and how much each UC is draining, but also to question whether patients still require a UC to remain in place. The educational programmes and implementation of protocols in improving UC care for patients is well proven. The difficulty is in maintaining the gains and entrenching the culture among health professionals.
Although staff shortages and competing priorities such as bed pressures always pose a challenge, health professionals continuously need to review different approaches for achieving the intended outcomes for high-quality patient care. Some of the practical approaches that can improve UC care in the clinical area are regular audits by senior nurses (matrons and ward sisters), regular spot checks on UCs, sharing audit and spot check results with the clinical team and empowering infection prevention link nurses.
Senior nurse audits, spot checks and informal education empower the healthcare team and promote continuous discussions to involve new members of staff. Although UC checklists are available in clinical areas, they are often tick-box exercises without an in-depth evaluation of the appropriateness of UCs. In addition to the senior nurse reviews and audits, empowering link nurses—who are perceived to be closer to the team than senior nurses—to continuously audit, challenge, prompt and create awareness go a long way to change the culture.
A catheter passport has been introduced in clinical areas at University Hospitals of Leicester NHS Trust for patients discharged from acute hospital with a UC. Although this scheme is in its infancy, district nurses the lead author has spoken to as part of her research have commended it highly because it seems to have improved communication. The passport makes them aware of when and why the UC was inserted and whether it is a short-term or long-term catheter. It saves them time from sometimes having to ring the clinical areas involved in the discharge of the patients for important information regarding the UC. Patients tend to have all the information about the UC in one place and feel well informed and involved in their care. The passports also improve awareness among family members who are then able to work collectively with the whole healthcare team, with the patient at the centre, to ensure appropriate insertion of the urinary catheter, effective care and appropriate UC days. Education for patients and carers regarding UC and adherence to hospital policy by healthcare workers are effective in reducing CAUTIs (Hu et al, 2015).
In summary, continuous informal and formal teaching sessions for health professionals, as well as regular audits and spot checks by senior nurses and link nurses, will lead to a continuous increase in knowledge, awareness and ownership among health professionals. Patients will be involved and at the centre of their UC care, resulting in reductions in CAUTIs, length of hospital stay and mortality in relation to UCs.
Conclusion
The most effective way to protect patients is to adhere strictly to infection prevention measures in relation to UCs, to write clear policies and guidelines on UC management, to institute sustainable educational programmes and to empower health professionals.
The holistic approach of putting the patient at the centre of the daily UC review, acknowledging the potential effects of CAUTIs, as well as the benefits of early removal and empathising with patients, could help to reduce incidence of CAUTI, reduce length of stay in hospital and mortality. While a UC remains in situ, it should be the responsibility of all healthcare workers, patients and relatives to continually ask the pertinent question: ‘Is this still required?’
KEY POINTS
- The longer a urinary catheter (UC) remains in the bladder, the greater the risk of the patient developing a urinary tract infection
- Complications of UCs include increased length of hospital stay and increased mortality
- Health professionals need to consider all other available options before inserting a UC
- The provision of continuing education programmes and regular audits empower health professionals to adequately assess the need for the insertion of UCs, and to continually monitor and remove the UC when it is no longer required
CPD REFLECTIVE QUESTIONS
- In your own clinical area, what are some of the measures you can take to ensure that urinary catheters are inserted appropriately for patients?
- Do you regularly review patients with urinary catheters and ask the question: ‘Is this urinary catheter still required?’
- Do you regularly assess the knowledge of staff regarding the effects of urinary catheters on patients and provide the necessary support?
- How do you ensure that health professionals in your clinical area receive regular updates and education on urinary catheters and their effects on patients?