

A key priority for UK Health policy-makers is to ensure the provision of good quality, evidence-based care for adults living in their own homes and communities, coupled with a clear desire to see the movement of care from acute-based settings to primary and community care (Department of Health and NHS England 2014; The King's Fund, 2014). District nursing (DN) services are fundamental to the delivery of proactive and preventative community-based care; however, changing demographics and an aging population, alongside increasingly complex health needs of patients, is placing significant demands on an already under-resourced and struggling workforce (The Queen's Nursing Institute (QNI) 2019). Often referred to as an ‘invisible workforce’ (Ball et al, 2014; National Assembly of Wales, 2019; QNI, 2019), undertaking work which is ‘some of the most complex of all’ (QNI, 2016; QNI 2019; Leary, 2019), DN services face additional challenges in articulating and demonstrating the complexity and skill of their care (Jackson et al, 2015). Historically, the ‘correct’ workforce for the population needs has been achieved more by ‘accident than by design’ (Reid et al, 2008).
Adequate workforce models that identify appropriate staffing levels for DN caseloads, which often fluctuate in numbers and acuity/dependency are lacking. The increasing complexity of care and changes in the needs of the population necessitates the need to ensure that workforce models are fit for purpose, enabling the right person, in the right place, with the right skills, to deliver care for patients.
Requiring an integrated and multi-disciplinary approach to caseload management of an increasing ageing population, combined with the desire to deliver robust population-based and person-centred healthcare services, it has never been more important to ensure that DN teams are sufficiently staffed and skilled. This article describes the journey of the All Wales DN Workstream in developing an evidence-based patient acuity and dependency tool to inform decisions on safe staffing levels in DN services through an iterative and Plan, Do, Study, Act (PDSA) change management approach.
Developing a draft patient acuity and dependency tool
The introduction of the statutory Nurse Staffing Levels (Wales) Act in 2016 led to the establishment of the All Wales DN Workstream. Under the overarching All Wales Nurse Staffing group, and in collaboration with Health Education and Improvement Wales (HEIW), these groups have worked to develop ‘Once for Wales’ – evidence-based, robust workforce methods and tools to inform decisions regarding staffing levels in DN teams.
Adopting the triangulation approach methodology of patient acuity, quality indicators and professional judgement, a key focus of the workstream was the development of a suitable patient acuity and dependency tool. This, alongside quality indicators and professional judgement, would offer district nurses the advice, guidance and definitions required to consistently assign individual patients to a ‘level of care’ by providing descriptions of the types of patients ‘typically seen’ at each level of care.
‘Patient acquity and dependency can be defined as ‘an estimate of the amount of care a patient requires based on the intensity, complexity and unpredictability of their holistic needs.’
The DN Workstream commenced by reviewing existing patient acuity and dependency tools already in use, including the Patient Complexity Instrument (Thomas et al, 2016) and the Safer Nursing Care Tool (The Shelford Group, 2014). Given the lack of suitable evidence-based DN patient and acuity tools, as well as a recognised value in ensuring a consistent approach to capturing patient acuity in nursing services across Wales, the All Wales DN Workstream decided to progress the development of a DN patient acuity and dependency tool named the DN Welsh Levels of Care tool (DN WLoC).
Taking an iterative approach through national engagement and workshop events, 600 district nurses participated in identifying over 1000 descriptors of care aimed at describing the specific holistic care needs of patients in the community. These initial descriptors were systematically and methodically developed through detailed examination, review and analysis over a 4-year period, resulting in the publication of the draft DN Welsh Levels of Care Tool (DN WLoC) in July 2022.
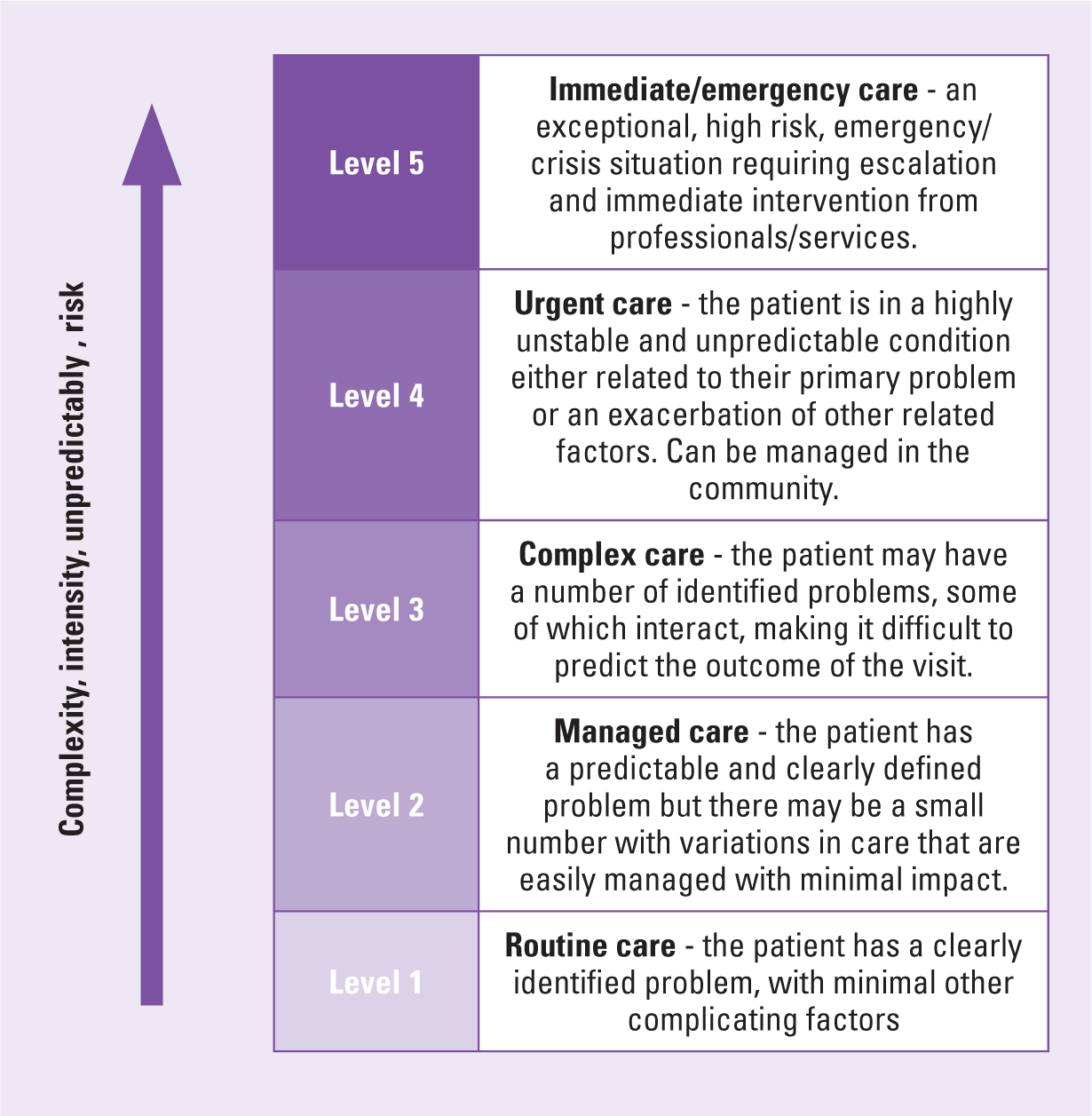
The DN WLoC tool consists of 5 levels of acuity (Figure 1):
- Level 5: Immediate/emergency care – an exceptional, high risk, emergency/crisis requiring escalation and immediate intervention from professionals/services
- Level 4: Urgent care – the patient is in a highly unstable and unpredictable condition either related to their primary problem or an exacerbation of other related factors. Can be managed in the community
- Level 3: Complex care – the patient may have a number of identified problems, some of which interact, making it more difficult to predict the outcome of the visit
- Level 2: Managed care – the patient has a predictable and clearly defined problem but there may be a small number of variations in care that are easily managed with minimal impact
- Level 1: Routine care – the patient has a clearly identified problem, with minimal other complicating factors.
The tool provides guidance on how nurses can use the DN WLoC alongside their professional judgement to assign their patients into the right level of care, by providing descriptions of the types of typical patient at each level of care (Figure 2). These descriptions are further broken down into categories with increasing specificity to summary descriptors, lay descriptors, clinical descriptors and nursing themes.
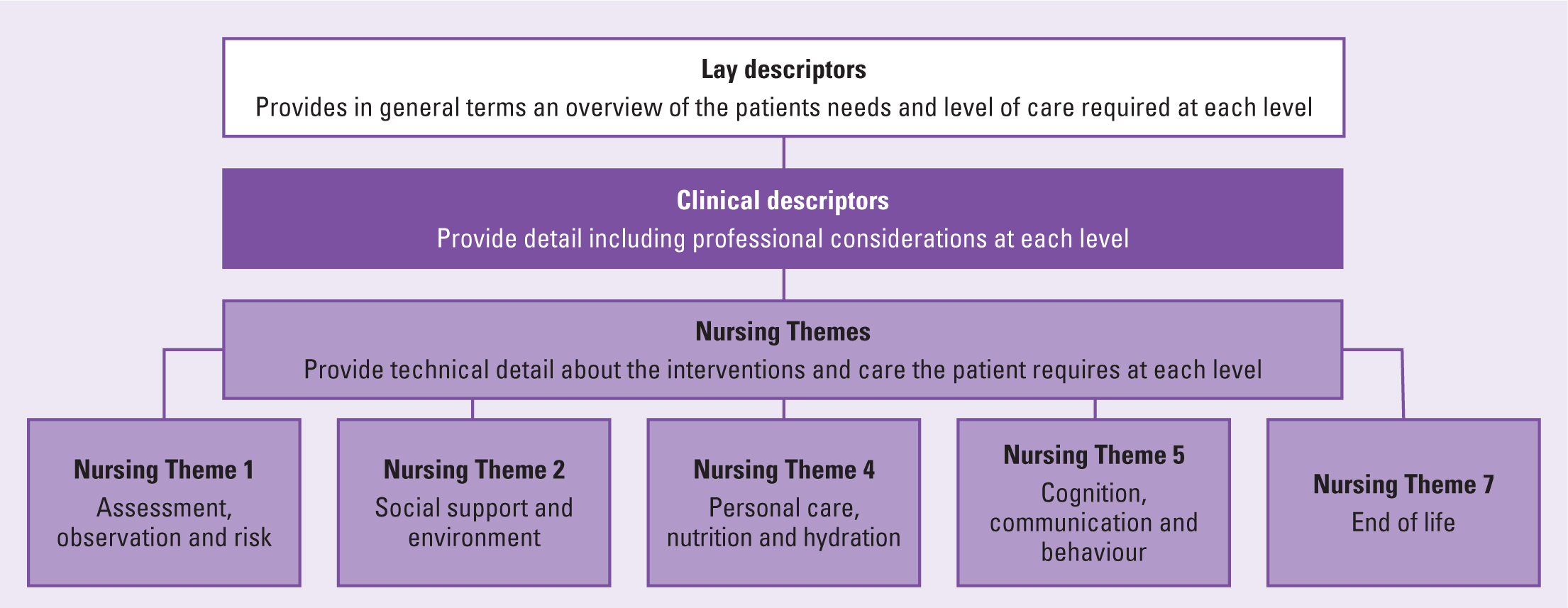
Each of these descriptors were developed through detailed examination and iteration with a wide range of DN staff from all levels of experience. They are designed in such a way that the categories are coherent across the five levels of care, leading to nurses attributing the right level of care to the right patient in a consistent manner.
Testing and piloting of the draft Tool
The COVID-19 pandemic was at the height of its second wave when testing of the draft tool commenced. While operational pressures limited the scale of testing, the commitment of members of the DN Workstream and DN teams across Wales was evident by the support, enthusiasm and engagement demonstrated.
Purpose
The purpose of the pilot was to determine whether the draft DN WLoC tool would enable district nurses to describe and evidence the acuity and dependency of patients on their caseload, using the tool to support their professional judgement and to consistently measure patient acuity.
Design
An explorative approach was taken for the pilot. Due to significant operational pressures across DN teams during the COVID-19 pandemic, the pilot was limited to three separate days over a 2-week period in June 2021.
Sample
Taking an inclusive approach to testing, all health boards in Wales were invited to participate in the pilot, and to ensure a representative sample, participants were required to be registered nurses working in Welsh DN teams. Participants varied in terms of skill mix and experience, with representation from newly qualified nurses to experienced district nurses. Their working environment and geographical localities included rural, urban, coastal and valley (post-industrial) settings. All participants attended training on the use of the DN WLoC tool prior to commencement of the pilot.
Patient cohort
- All patients who were on an active DN caseload and visited by the participants on three separate days over a 2-week period in 2021
- No patient exclusions were identified
- No patient participation was required for the Phase two of the pilot study.
Data Collection
The lack of a national IT system limited options for data reporting, collection and evaluation across both phases of the pilot. For the initial phase of the pilot, Microsoft Forms was used to undertake a questionnaire approach to data collection. This led to the creation of two forms: form one, which required participant demographic data, and form two, which required participants to provide patient-related information from a combination of drop-down boxes and free text answers. Participants were asked to allocate acuity and dependency scores using the Welsh level of Care tool on every patient they saw on each of the three days.
Following the success of the first phase of the pilot which looked at the usability of the tool by district nurses in practice, the second phase of the pilot considered the validity and reliability of the tool in practice. All participants who had engaged in the initial training for phase one were invited to participate in this second phase (n=103); however, the impact of COVID-19 and resulting operational pressures meant that participation in this second phase was limited with only 21 participants (20%) engaged.
Participants were asked to review the summary, lay or clinical descriptors, to agree or disagree with the level of care attributed to the case during phase one. A data capture sheet was developed to allow participants to read the information provided for each case study and using their professional judgement and the DN WLoC tool, decided if they agreed with the acuity level previously recorded.
Overall, 20 case studies from the 1433 original scores were chosen for this phase and reflected a mix of scores from across the levels of care – L5 (1), L4 (1), L3 (4), L2 (8), L1 (6). The data capture form provided drop down boxes for each of the participants to choose whether they agreed with the original score, disagreed with the original score or felt there was not enough information to provide an answer. Options for free-text comments were also provided and participants were asked to record any reasons for disagreement and what level they would have chosen instead.
Results
The findings from phase one are outlined below (Tables 1,2 and 3):
- A total of 103 staff were recruited to participate in the pilot
- Some 87 participants submitted patient acuity levels (85% of participants)
- Of these, two participants were newly qualified, while most participants had been qualified >6 years
- A total of 1433 patient acuity levels were documented
- Of the 1433 patient acuity levels generated, majority of patients (42.6%) were classed as level two (managed care), followed by level one (routine care (30%) and level three (complex care (20%))
- There were relatively low numbers of patients classed as either requiring immediate/urgent care at level five (1.3%) and level four (5.7%)
- The most common age group for visits were between 81–85 years of age
- A total of 91% of visits were for scheduled care, while 88% of visits were for follow up
- Treatment (care delivery) was the main reason for visits
- Wound care accounted for 41% of interventions, while 86% of participants thought the WLoC tool was easy or very easy to use.
Table 1. Welsh Levels of Care Tool (WLOC) scores allocated per level
| NHS Wales % | WLoC |
|---|---|
| 1.3% | 5 |
| 5.7% | 4 |
| 20.4% | 3 |
| 42.6% | 2 |
| 30.0% | 1 |
Table 2. Types of interventions provided on visits
| Clinical conditions | No (%) |
|---|---|
| Wound care | 592 (41) |
| Medication | 482 (34) |
| Pressure area care | 442 (31) |
| Chronic disease | 222 (16%) |
| Palliative care | 153 (11%) |
Table 3. Suggested interventions in phase one
| Intervention | No (%) |
|---|---|
| Treatment/care | 1245 (88) |
| Advice | 731 (51) |
| Assessment | 727 (51) |
| Evaluation | 519 (36) |
| Monitoring/screening | 466 (33) |
| Education | 309 (22) |
| Referrals | 145 (10) |
In phase two, 20 participants reviewed 20 case studies (Table 4):
- Of all responses for each case study 76.5% (n=400) of responses agreed with the original score, 13.5% (n=54) responses disagreed and 10% (n=40) stated there was not enough information to decide
- The highest variance in agreement was found in case studies relating to level two acuity
- Some of the responses suggested there was some confusion over use of the tool; for example, the acuity score provided was disagreed with by two participants on the basis of whether a registered or unregistered nurse was attending or not, rather than on the acuity of the patient's condition and risk, suggesting misunderstanding by the participants rather than the tool not being appropriate for use.
Table 4. Outcomes from case study reviews of the Welsh Levels of Care Tool
| WLOC case study | Number of case studies | % of Agree responses | Disagree | Not enough information |
|---|---|---|---|---|
| Level 5 | 1 | 85% (n=17) | 0% | 15% (n=3) |
| Level 4 | 1 | 65% (n=13) | 0% | 35% (n=7) |
| Level 3 | 4 | 73.75% (n=59) | 11.25% (n=45) | 15% (n=12) |
| Level 2 | 8 | 76.25% (n=122) | 18.13% (n=29) | 5.65% (n=9) |
| Level 1 | 6 | 80% (n=95) | 13.33% (n=16) | 7.5% (n=9) |
Discussion
Although a relatively small scale pilot, the objectives and aims were achieved. The pilot demonstrated that the tool was applicable in practice by district nurses with limited but positive findings in the reliability and validity of the tool when applied in clinical practice.
Feedback across the seven nursing themes identified concerns that there was some duplication, which may result in a lack of consistency in using the document. In response, further workshops were held in April and May 2022 where themes were systematically reviewed. Overall, two themes were identified as suitable for amalgamation as there was felt to be an amount of duplication in descriptors; with the original ‘breathing’ and ‘medication’ themes being incorporated into the ‘assessment, observation and risk’ theme.
Following these changes, a revised document with five nursing themes was formally agreed for use as a working document and the DN WLoC was rolled out across Wales from November 2022.
During the period of the tool being developed, DN teams in Wales also adopted the Civica scheduling system, which supports teams to provide intelligent scheduling of patients and caseloads. Following the success of the DN WLoC pilot, the Civica scheduling system was adapted to incorporate the tool, enabling community and district nurses to record patient acuity scores in real time, as well as being able to see recent trends in patients' acuity and dependency.
District nurses enter the patients' acuity score (either during or after the visit) into the Civica mobile app or web-based application. Both current and the previous three levels of care are accessible in the patient record, with acuity and workforce data collated and displayed through analytical dashboards. The datasets can be viewed through various fields such as team or healthboard-wide levels of care, reporting periods and workforce data, enabling teams and healthboards to use the data to plan workforce needs. Ongoing evaluation and updates to the Civcia system are supported and continue to evolve as staff and teams become more familiar with the data and systems.
The purpose of this tool is to provide nursing teams with the advice, guidance and definitions required to consistently assign individual patients to a level of care. The DN WLoC tool has been shown to provide a consistent means of measuring and evidencing the acuity and dependency of individual patients and the caseload. DN teams have reported that this information is essential to informing decisions regarding the day-to-day deployment of nursing staff and members of the multi-professional team, to ensure that the needs of patients are met and to inform local and national workforce planning. Information on patient acuity, patient need, and demand is being found to provide valuable insight, which can be used to inform the delivery of services and enable local and national benchmarking.
The development of this national tool is a significant achievement for the DN workstream and testament to the commitment and hard work of all those involved, who have strived to develop a national tool that will help to inform the delivery of safe and effective patient care and services.
Limitations
The pilot was not without significant challenges and limitations, none more so than the ongoing COVID-19 pandemic and the impact on operational services. Due to operational pressures, both the size of the pilot and the testing time were limited, and it was acknowledge that a wider roll out of the tool would enable continuous data capture across all DN teams.
Limitations
The scope of the pilot was limited to testing the useability and validity of the tool, focussed on whether the participants could determine the acuity and dependency of a patient on their caseload using the DN WLoC tool. Further evaluation of the tool and data will increase understanding and applicable knowledge taken from the acuity levels in correlation to team location, staffing levels or skill mix. The lack of a national IT system for data capture across Wales made collection and analysis of the pilot data challenging. The use of MS Forms and Excel were used as it offered simple, quick access to all NHS users with an email address; however, the subsequent development of the Civica system as a means of recording and analysing WLoC data has since mitigated many of the pilot challenges.
Conclusion
The literature reviewed demonstrates that there is a need for DN services to be able to define and measure the acuity and dependency of caseloads to determine adequate and sensitive nurse staffing levels. This article described the iterative approach which was taken to both developing and testing the DN WLoC in clinical practice. While the results of the pilot demonstrate that the tool is applicable for use in clinical practice, further evaluation and review is needed to determine the validity and consistency of the tool. A formal evaluation of both the tool and the additional data provided by Civica will be undertaken in November 2023 with the ambition that results will contribute and influence both real time and future workforce planning, as well as nurse staffing levels for community and DN teams.
Key points
- The Welsh Levels of Care document is a national tool to measure patient acuity and dependency, not an operational process to be followed from beginning to end each time a patient is assessed
- Nurses are required to make a professional judgement about their patients' level of acuity and this document is simply to provide nurses with sufficient information to validate that judgement
- Until this tool was developed there was not a national standardised tool within district nursing to measure patient acuity and dependency
- For district nurses, a level of care is attributed to a patient at every visit (face to face or virtually) to capture patient acuity at the time the nurse has assessed them.
CPD reflective questions
- How can district nursing demonstrate the increasing complexity and challenges of caseload managements and workforce recruitment and retention?
- How may acuity and dependency tools help with caseload management in district nursing?
- How does professional judgement impact on using acuity and dependency tools?
- IT systems in district nursing are often found to be insufficient - what IT systems or tools would help with caseload and workforce management?