

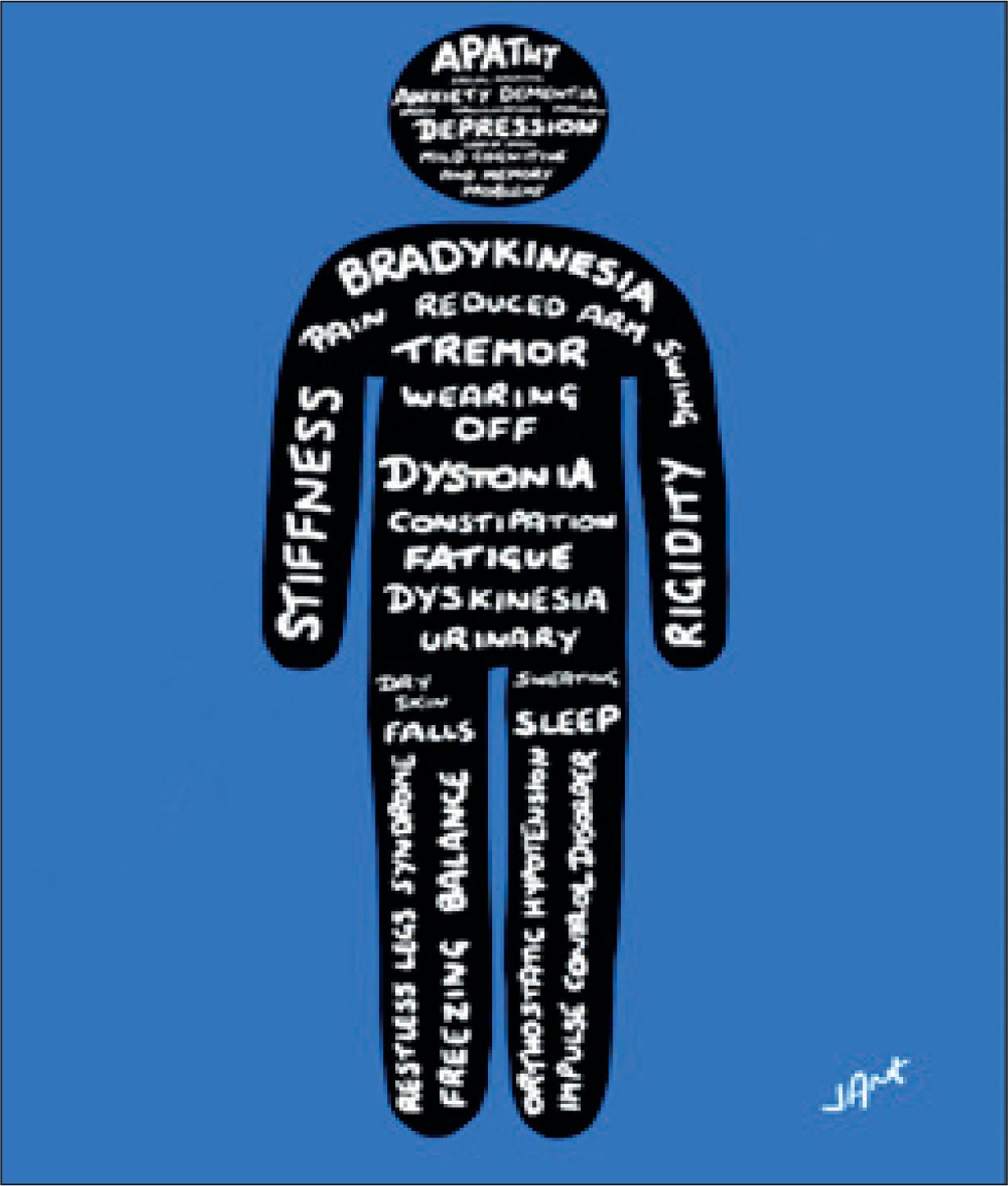
Parkinson's disease is a progressive neurological disease, causing motor problems that include rigidity, slowness and tremor, and a range of non-motor symptoms that impact mood, cognition, gastrointestinal function, speech and swallowing (Figure 1).
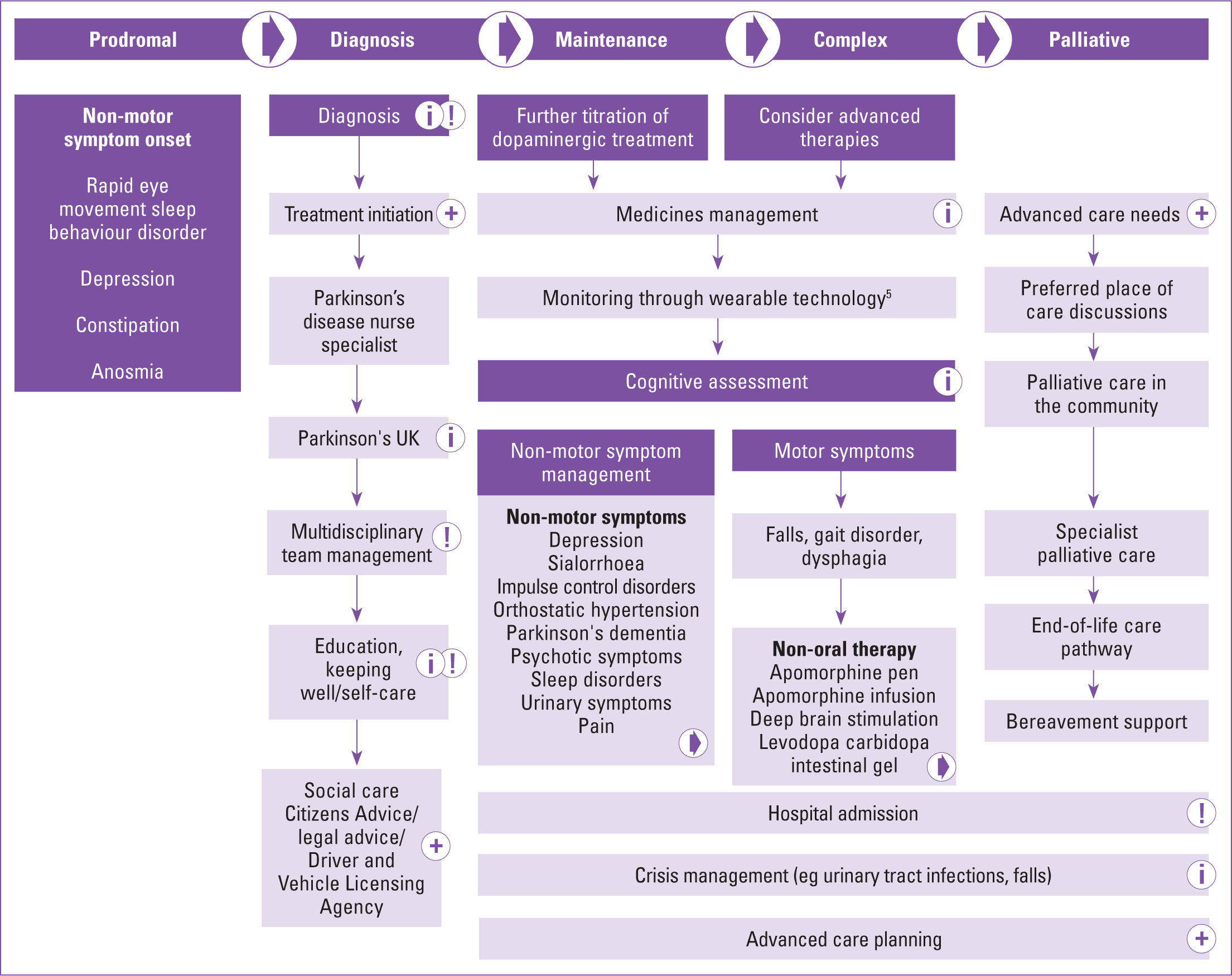
More than 6 million individuals worldwide have Parkinson's disease (Armstrong, 2020), with more than 145 000 people in the UK living with the condition at present (Parkinson's UK, 2018). The condition progresses over time and has been categorised into four stages: diagnosis, maintenance, complex and palliative (MacMahon and Thomas, 1998; Peel, 2013). Figure 2 shows the stages clearly depicted in the non-oral therapies pathway, with the addition of the prodromal phase (Kobylecki, 2020).
An audit by Parkinson's UK (2019) found that complex and advanced Parkinson's was found to affect one-third of the Parkinson's population, meaning up to 48 000 people could potentially require one of the non-oral therapies: apomorphine, deep brain stimulation (DBS) or levodopa carbidopa intestinal gel (LCIG). Demographic changes, the rising incidence of Parkinson's (Parkinson's UK, 2018a) and the increasing likelihood of comorbidities as Parkinson's progresses (Santos García, 2017) all mean that community nurses will often be required to support the growing needs of these individuals.
The Parkinson's non-oral therapy pathway was originally launched in 2016 to clarify the complex access to non-oral treatments for Parkinson's disease, and a new version of the pathway provides updated schematics for assessment and treatment of the initial three non-oral therapies, as well as advice on management of sialorrhea (drooling), which can have a significant impact on someone's quality of life (Neurology Academy, 2021).
With appropriate and timely access to the right medication therapies, individuals experiencing a complex disease state and requiring a high level of care and support can revert back to a level where they have more independence, greater quality of life, and fewer care requirements (MacMahon and Thomas, 1998).
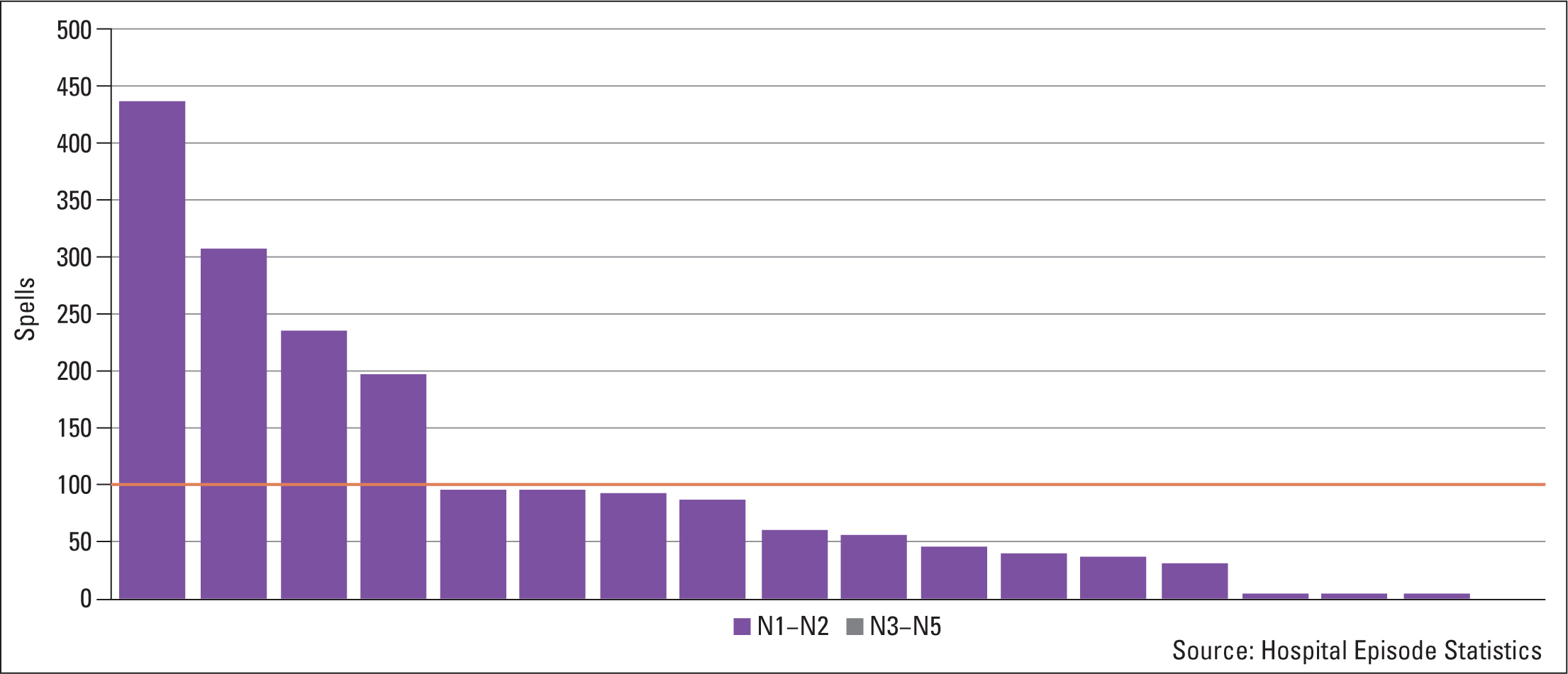
The most recent evidence from service audits (Parkinson's UK, 2019) and Hospital Episodic Statistics (HES) data (Fuller, 2021) highlight that there is still inequity of access to non-oral medication for Parkinson's patients across the UK, while data shows a significant decline in the number of people accessing DBS between 2016 and 2019 (Figure 3).
Additional evidence suggests that this inequity and impacted access has been exacerbated by the effects of COVID-19 (Parkinson's Academy, 2020), with a number of services reporting an inability to begin or continue non-oral treatments during the early months of the pandemic.
Community nursing roles in complex therapies
Although specialist healthcare practitioners are required to conduct assessments for these therapies, early recognition that a patient with Parkinson's might benefit from a non-oral therapy is an important first step in the journey. It is often the case that community nurses, who may see a patient regularly as their condition progresses, will become aware of a person's changing needs and are well-placed to make a referral to their local specialist nurse or Parkinson's team to ensure that patient is reviewed in a timely manner (Maybin, 2016; Royal College of Nursing and Queen's Nursing Institute, 2019).
Aside from identifying patients who may need specialist assessment for a non-oral therapy, the aftercare around patient education, monitoring and management in non-oral therapies can be significant (Neurology Academy, 2021). Community and district nurses are instrumental in providing good aftercare, such as the appropriate use of equipment, monitoring for adverse reactions and potential complications, and are often best placed to support the patients' education around their own safety monitoring and management (Maybin, 2016).
Identification and early referral
District and community nurses can identify early on whether specific non-motor symptoms are impacting a person's daily living and become familiar with certain tools, such as the non-motor symptom questionnaire (Chaudhuri, 2006), which can help nurses to identify these (Table 1). Non-motor symptoms are commonly experienced throughout the disease trajectory, but become more prevalent as the condition becomes more severe (Rodriguez-Blazquez, 2020). As previously mentioned, one such non-motor symptom is drooling, or sialorrhea (Neurology Academy, 2021).
Table 1. Non-motor symptoms in advanced or complex Parkinson's disease
| Category of non-motor symptoms | Non-motor symptoms |
|---|---|
| Neuropsychiatric | Mood disorders (eg anxiety, depression)PsychosisDementia |
| Autonomic | Bladder and bowelSpeechSwallowingNauseaDrooling (sialorrhea)Dysphagia |
| Sleep | Disrupted sleepInsomniaRapid eye movement sleep behaviour disorder |
| Sensory processing | PainSensory disruptionNutrition, weight loss or gain |
Note: Taken from the Parkinson's Tailored Management virtual course for nurses (Parkinson's Academy, 2021a)
The pathway provides helpful top-level prompts for assessing whether a person with Parkinson's might benefit from a non-oral therapy, such as the ‘5-2-1’ tool, which community nurses could keep in mind when seeing the person in their home (Figure 4).
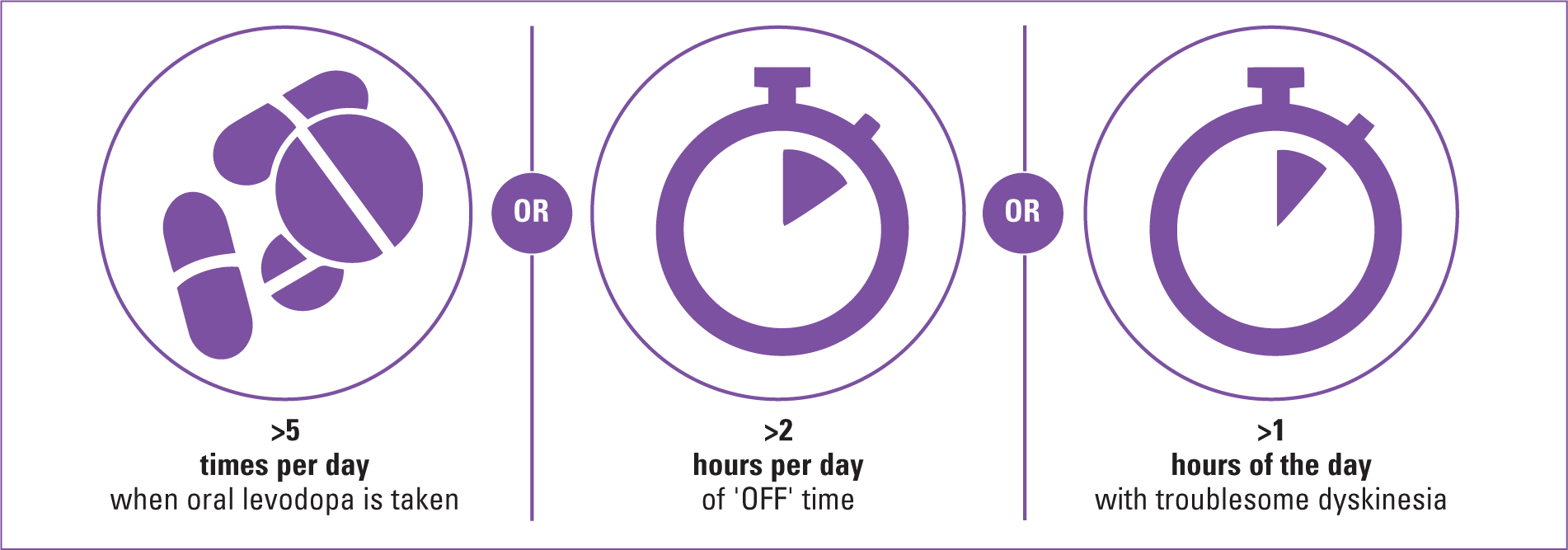
The ‘5-2-1’ prompt helps in the process of considering referral for non-oral therapy based on the amount of time a person is ‘on’ (experiencing well-controlled symptoms) or ‘off’ as a result of their medication (Parkinson's UK, 2018b). This on/off state is often used to refer to motor symptoms, but can be experienced as significantly with non-motor symptoms (Martínez-Fernández, 2016).
Although individuals with Parkinson's are likely to have an annual medication review, community nurses may become aware of a change when attending patients in their home and can escalate the need for a medication review, so that their needs are responded to in a more timely and effective manner.
Aftercare, monitoring and patient education
With aftercare and monitoring, each therapy requires different focus, and familiarisation with these could improve both professional confidence and patient care.
Apomorphine
Apomorphine is a dopamine agonist derived from morphine, but without opiate properties. It is not a controlled drug, and is administered via subcutaneous intermittent injection (‘pen’) or continuous infusion (‘pump’). Community and district nurses, supported by their local Parkinson's specialist, are essential in supporting patients in appropriate use and safety management when using either pump or pen, with successful outcomes associated with both the drug response and the patient's understanding of how to manage their therapy (Bhidayasiri, 2016).
Community nurses may be instrumental in noticing any early warning signs that treatment ought to be discontinued. The Parkinson's non-oral pathway highlights several reasons to discontinue use of the apomorphine pump (Parkinson's Academy, 2021b). These include:
- Severe nodules
- Postural hypotension
- Patient choice
- Worsening cognitive issues
- Psychosis leading to delusions
- Emaciated frail patient
- Patient fatigue
- Need for alternative therapy (eg levodopa carbidopa intestinal gel or DBS)
Deep brain stimulation
DBS is a surgical procedure in which very fine electrodes are implanted into specific anatomical pathways in the brain to influence neural signalling pathways that have been affected by conditions like Parkinson's. These electrodes are connected to a stimulator embedded subcutaneously under the collar bone and controlled by a linked handheld device that the patient has access to, installed with set parameters.
Although DBS is managed carefully by the local specialist team who, after the surgery, will be monitoring the patient closely for complications or interactions, it may be that a community nurse may notice a complication before the patient or specialist does. The Parkinson's Tailored Management course (Parkinson's Academy, 2021a) covers DBS in detail (module 1, session 6) and lists a number of complications for nurses to be particularly vigilant of in people with Parkinson's following their DBS surgery (Table 2).
Table 2. Possible complications to monitor for in Parkinson's patients post-deep brain stimulation surgery
| Possible complications | Possible interactions |
|---|---|
| Risk of infection | Contact sports or hobbies interacting with the hardware, such as rugby, boxing and martial arts |
| Dysarthria and dysphagia (these can occur with Parkinson's progression and may be exacerbated by deep brain stimulation (DBS)) | Knowing when to ‘switch off’ where hardware may interfere with another treatment |
| Postural instability (may occur naturally or be exacerbated by DBS—hardware must be checked when falls occur) | |
| Tendency towards apathy or impulse control disorder (Baig, 2019) |
Note: Taken from the Parkinson's Tailored Management virtual course for nurses (Parkinson's Academy, 2021a)
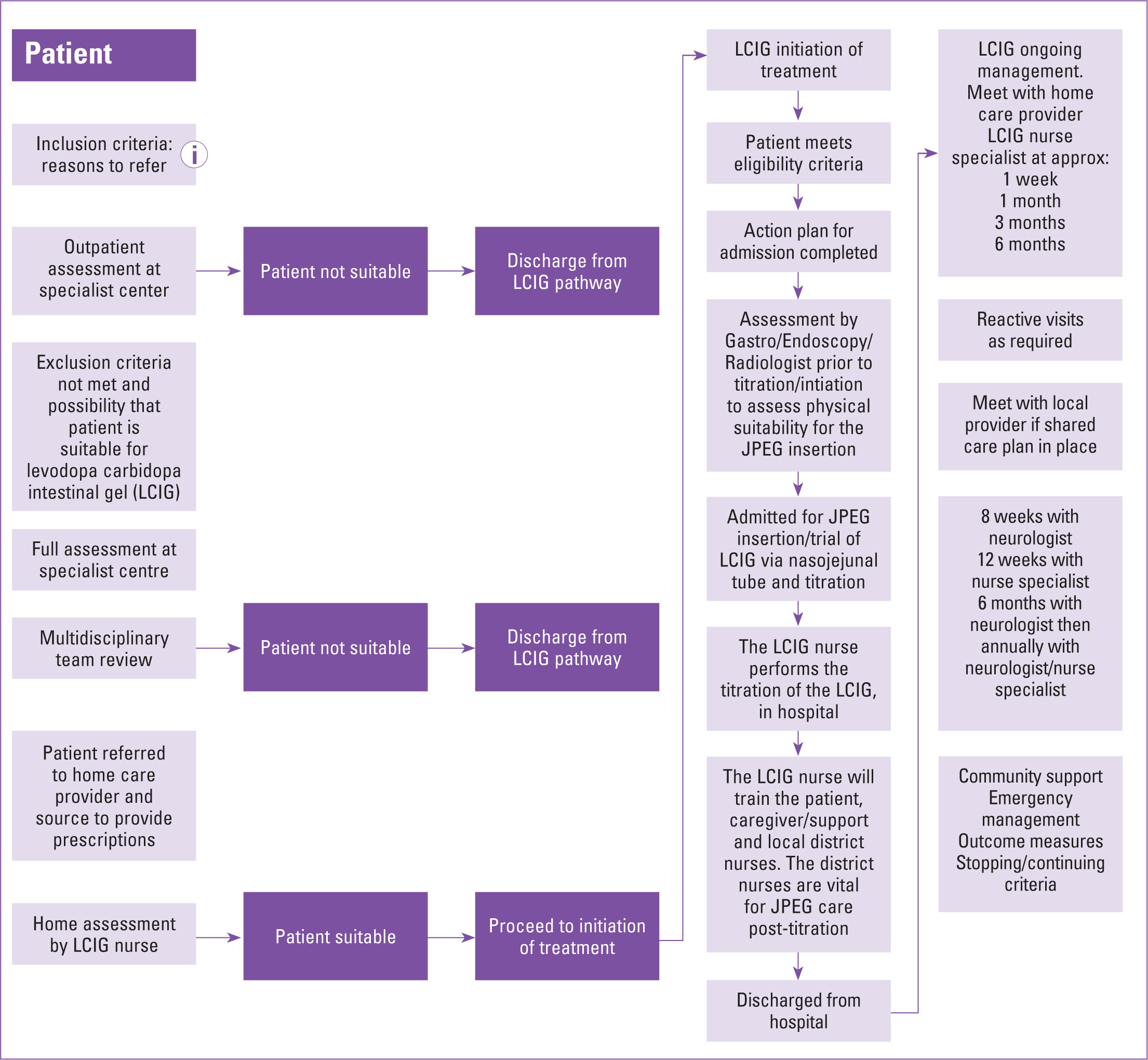
Levodopa carbidopa intestinal gel
Levodopa carbidopa intestinal gel (LCIG) bypasses the stomach and avoids the effects of delayed or slow gastric emptying to provide a stable levodopa concentration. This can give increased daily ‘on’ time without increased dyskinesia, while reducing ‘off’ time.
LGIG requires the insertion of a jejunum percutaneous endoscopic gastrostomy (JPEG) tube. One of the key areas requiring monitoring is the JPEG site. The tubing is held in place by a device called a bumper (fixed on either side of tube entry). Supporting Parkinson's patients to keep the area clean, reduce risk of infections, and ensure the pump is running well may all be required of community nurses. Particular mitigation against, or early detection of, ‘buried bumper syndrome’(BBS), may also be needed. BBS is a severe complication where the internal ‘bumper’ moves, sometimes due to excessive tissue compression between the external and internal ‘bumpers’. Early warning signs that this may be occurring include leakage, inability to insert, and loss of patency, often seen as a trio of symptoms (Cyrany, 2016). This occurs more frequently in patients with LCIG than in those receiving enteral feeding, and it needs careful monitoring, particularly as BBS does not result in treatment failure in Parkinson's patients, making it more difficult to detect (Spanaki, 2021).
The specialist overview pathway (Figure 5) clearly highlights the need for training from the LCIG nurse to local caregivers and district nurses before a patient may be discharged from hospital following their procedure to use LCIG.
Sialorrhea
Sialorrhea, or drooling, is a problem that many people with Parkinson's experience; while it has been historically underrecognised, it is ranked by patients as one of the most debilitating problems in Parkinson's disease (Isaacson, 2020). Caused by the effects of Parkinson's rather than by producing more saliva, difficulty in swallowing or stooped posture can make saliva management harder. This can have a significant impact on quality of life and socialisation, and can affect confidence in eating and communicating (Cotton, 2021).
Advances in medications, when supported by simple aids and modifications, can make a huge difference to those experiencing sialorrhea, and the non-oral pathway provides a helpful framework for identification, management and treatment (Parkinson's Academy, 2021b).
Community or district nurses can use the Drooling Severity and Frequency Scale (DSFS) (Table 3) to assess whether the patient might benefit from a referral for specific treatment or more supportive management via speech and language or occupational therapy. Nurses may also be able to support patients in following advice around postural changes and use of aids to manage this debilitating symptom.
Table 3. Drooling Severity and Frequency Scale (DSFS) outlined in the Parkinson's Non-Oral Pathway
|
|
|---|---|
| Drooling severity score | Drooling frequency score |
| 1. Dry (never drools) | 1. Never |
| 2. Mild (wet lips only) | 2. Occasionally |
| 3. Moderate (wet lips and chin) | 3. Frequently |
| 4. Severe (clothing becomes damp) | 4. Constantly |
| 5. Profuse (clothing, hands, objects become wet) | |
Conclusion
Given demographic changes, the number of people with Parkinson's is likely to increase, and the complexity of the condition means that community nurses will undoubtedly have people with Parkinson's on their caseloads.
Familiarisation with a best practice pathway approach, recognition of early indicators that a person with Parkinson's may benefit from a non-oral therapy, and clarity around optimal aftercare and monitoring among community and district nurses can ensure people with Parkinson's are well supported and that any complications or difficulties are reduced through the earliest possible intervention.
Key points
- Demographic changes mean community nurses will undoubtedly see more people with Parkinson's as part of their caseload
- Earlier recognition of the complex phases of the condition and need for non-oral therapies will result in improved and more timely care for individuals with Parkinson's disease
- An integrated pathway approach to care will ensure community nurses can confidently support optimal management of their Parkinson's patients